Congrats to the jurisdictions that successfully submitted their CDC PS19-1906 application. Here are some of NMAC’s thoughts about the next steps for leaders working on the plan: Don’t wait. The turn-around time for your jurisdictional plan to end the HIV epidemic is short and waiting will make the job harder. Prior to receiving the final funding award, NMAC believes it is important to:
Congrats to the jurisdictions that successfully submitted their CDC PS19-1906 application. Here are some of NMAC’s thoughts about the next steps for leaders working on the plan: Don’t wait. The turn-around time for your jurisdictional plan to end the HIV epidemic is short and waiting will make the job harder. Prior to receiving the final funding award, NMAC believes it is important to:- Inform your governor, mayor, and other elected officials about your planning efforts to end the HIV epidemic in their jurisdiction,
- Work to identify planning body members, and
- Finalize your jurisdiction’s epi profile.
 Since plans are focused in particular jurisdictions, it will be important to inform, educate and seek support from city, county, state and federal elected officials. Their support is critical as plans are implemented. Not only do they help carry the message, federal elected officials vote on the 2021 Federal Budget that will hopefully include implementation funding for our important work to end an epidemic. The goal is to reduce new HIV cases by 75% in five years and we need elected officials on our side.House Appropriations Subcommittee Language
Since plans are focused in particular jurisdictions, it will be important to inform, educate and seek support from city, county, state and federal elected officials. Their support is critical as plans are implemented. Not only do they help carry the message, federal elected officials vote on the 2021 Federal Budget that will hopefully include implementation funding for our important work to end an epidemic. The goal is to reduce new HIV cases by 75% in five years and we need elected officials on our side.House Appropriations Subcommittee LanguageWhen putting together new planning bodies or using existing councils, health departments should remember the House’s subcommittee on appropriations language (see below):
Community-Based Organizations. —The Committee recognizes that community-based organizations play a crucial role because of their capacity to reach communities highly impacted by HIV. The Committee directs CDC to ensure that planning councils reflect their local epidemic by including community-based organizations and people living with HIV. The Committee further requests CDC’s progress of engaging such communities be included in the fiscal year 2021 Congressional Budget Justification.
Planning Bodies Should Reflect Their Local HIV Epidemic
 While not final, the House requested that the planning bodies reflect their local HIV epidemic. They also requested a progress report about the role of community-based organizations in the CDC’s 2021 Congressional Budget Justification. This means Congress will monitor how CDC engages community. NMAC supports this action and will work with planning councils to make sure they meet Congress’s expectations. NMAC asks CDC to track demographic information on planning council members by HIV status, PrEP status, race, gender, gender identity, zip code, and sexual orientation. For most health departments these stats are a given; however, it’s not true for every jurisdiction. Zip codes are important because they often divide regions along lines of economics, race, sexual orientation, and health services. HIV programs should be targeted to the zip codes with the largest number of PLWH. People who live in wealthier zip codes tend to have easier access to services that are missing in poorer communities. These are minimal standards and planning bodies should expand what demographics are to be shared based on their jurisdiction’s data sets and needs.
While not final, the House requested that the planning bodies reflect their local HIV epidemic. They also requested a progress report about the role of community-based organizations in the CDC’s 2021 Congressional Budget Justification. This means Congress will monitor how CDC engages community. NMAC supports this action and will work with planning councils to make sure they meet Congress’s expectations. NMAC asks CDC to track demographic information on planning council members by HIV status, PrEP status, race, gender, gender identity, zip code, and sexual orientation. For most health departments these stats are a given; however, it’s not true for every jurisdiction. Zip codes are important because they often divide regions along lines of economics, race, sexual orientation, and health services. HIV programs should be targeted to the zip codes with the largest number of PLWH. People who live in wealthier zip codes tend to have easier access to services that are missing in poorer communities. These are minimal standards and planning bodies should expand what demographics are to be shared based on their jurisdiction’s data sets and needs.
Policies and Procedures for Operation
 When putting together your planning bodies, it will be important to determine policies and procedures for operation in advance of the selection process. To some this might seem insignificant, but there are people of color leaders who believe systems like Robert’s Rules of Order are a racist construct meant to minimize our voice. It is important that planning councils’ policies and procedures empower the communities the jurisdictional plans need to reach. NMAC believes race and our ability to reach people of color is core to the solution. If we include systems that are experienced as oppressive, then how can community believe in the solution.
When putting together your planning bodies, it will be important to determine policies and procedures for operation in advance of the selection process. To some this might seem insignificant, but there are people of color leaders who believe systems like Robert’s Rules of Order are a racist construct meant to minimize our voice. It is important that planning councils’ policies and procedures empower the communities the jurisdictional plans need to reach. NMAC believes race and our ability to reach people of color is core to the solution. If we include systems that are experienced as oppressive, then how can community believe in the solution.
Jurisdiction’s Epi Profile
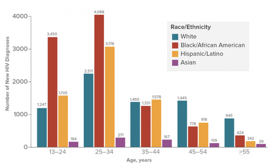
Your jurisdiction’s epidemiological (epi) profile should be the foundation for program and funding decisions. As a result, everyone should be informed and educated about this critical information. Community needs access to HIV statics that include the race, gender, gender identity, sexual orientation, and zip codes for the people living with HIV and people on PrEP in their jurisdictions. Most jurisdictions have this data but NMAC is concerned the information is not available in all jurisdictions. This is the minimum data to be shared. Planning councils may ask for more information like community viral load, and STDs and Hepatitis overlays. NMAC believes that work to end the HIV epidemic should also include work to end STDs and Hepatitis.
Treatment Education for Planning Body Members
 Planning council members must be knowledgeable about all the components of their jurisdiction’s plan, particularly information about U=U, PrEP and their epidemiological profiles. Often data is too technical and not understood by people without graduate degrees. Our movement has lost much of its community treatment education infrastructure. NMAC believes treatment education is core to supporting planning council members, PLWH, and people on PrEP to understand the value of retention in healthcare and adherence to meds. When people know better, they do better. NMAC calls on CDC and HRSA to support Planning Councils requests for treatment education services as tools for retention and adherence.
Planning council members must be knowledgeable about all the components of their jurisdiction’s plan, particularly information about U=U, PrEP and their epidemiological profiles. Often data is too technical and not understood by people without graduate degrees. Our movement has lost much of its community treatment education infrastructure. NMAC believes treatment education is core to supporting planning council members, PLWH, and people on PrEP to understand the value of retention in healthcare and adherence to meds. When people know better, they do better. NMAC calls on CDC and HRSA to support Planning Councils requests for treatment education services as tools for retention and adherence.
Organizing PLWH & People on PrEP
 It will also be important to support organizing by People living with HIV and People on PrEP. Peer to peer education and support is also key to adherence and retention. I don’t think the federal government wants to have the sex talk with PLWH or people on PrEP. This is better left to support groups organized for peer to peer learning and to help communities meet the goals of this initiative. Ways to organize should be left to local planning councils to determine. Some will organize along lines of race, gender, gender identity, or zip code, while others want to be part of groups that include everyone. There is not one right way to organize and communities should make their own priorities. These organized coalitions should be prioritized for the treatment education efforts noted above.
It will also be important to support organizing by People living with HIV and People on PrEP. Peer to peer education and support is also key to adherence and retention. I don’t think the federal government wants to have the sex talk with PLWH or people on PrEP. This is better left to support groups organized for peer to peer learning and to help communities meet the goals of this initiative. Ways to organize should be left to local planning councils to determine. Some will organize along lines of race, gender, gender identity, or zip code, while others want to be part of groups that include everyone. There is not one right way to organize and communities should make their own priorities. These organized coalitions should be prioritized for the treatment education efforts noted above.
There is lots to consider. This is the first of many e-newsletters that will suggest options for health departments to consider when putting together their jurisdictional plans. We invite everyone to send additional recommendations to Linda H. Scruggs, the director of NMAC’s Training Center to End the Epidemic. Successful planning requires that all communities highly impacted by HIV have a real seat at the table. Far too often only lip service is provided to this important need. If you are unclear about how to proceed, ask for help. Nobody has all the answers, but it’s better when we work collaboratively. NMAC is committed to your success and we are here to serve.
Yours in the struggle,
Paul Kawata
30 Years of Service