NMAC is changing the name of the United States Conference on AIDS to the United States Conference on HIV. AIDS is considered stigmatizing language to many people living with HIV and the last thing we want to do is add to their discrimination. This is especially important because we need to reach 500,000 more people living with HIV if we want to end the domestic epidemic. Please watch this important video about the 2020 meeting!
NMAC is changing the name of the United States Conference on AIDS to the United States Conference on HIV. AIDS is considered stigmatizing language to many people living with HIV and the last thing we want to do is add to their discrimination. This is especially important because we need to reach 500,000 more people living with HIV if we want to end the domestic epidemic. Please watch this important video about the 2020 meeting!
Join us October 10-13 in San Juan, Puerto Rico. The web site for the 2020 USCH is now live! The 2020 theme is Luchando Por Nuestras Vidas (Spanish for Fighting For Our Lives). The theme honors our past and speaks to the future. Unfortunately, luchando por nuestras vida is what the people of Puerto Rico do daily. The theme also speaks to the struggle facing people living with HIV and people on PrEP. We are all connected in the fight for a fair and just world.
 The 2020 meeting will serve Puerto Rican and US Virgin Island realness to educate about the challenges of reaching people who speak different languages or have different cultures and values.
The 2020 meeting will serve Puerto Rican and US Virgin Island realness to educate about the challenges of reaching people who speak different languages or have different cultures and values.
The 2020 meeting is in San Juan to 1) provide economic development in a country devastated by Hurricane Maria and the recent earthquakes, 2) give attendees the experience where English is not the primary language, and 3) learn about the rich Puerto Rican and US Virgin Island cultures as a way to value differences.
This image of doors in Old San Juan gets at the message for this meeting. We are all different and beautiful in our own way. Our movement is about the diversity of the doors and how to value and honor differences.
San Juan Convention Center

In order to hold the meeting in San Juan, we had to move to the Puerto Rico Convention Center. It is the only site big enough for USCH. I was just there for a planning meeting with the Puerto Rico Host Committee. They are so excited to share their story of overcoming the challenges of weather, earthquakes, and HIV.

Just in time for USCH, a new entertainment center, El Distrito, will open next to the convention center. El Distrito will have inexpensive dining options, a movie theater, concert hall and an Aloft hotel. Phase I of the complex is slated to open in March.
Registration
Registration is now open. You must register before you can make your hotel reservation if you want to be part of the conference block. Early bird registration fees are $490 for NMAC members and $625 for non members.
Hotel Accommodations
There are no hotels big enough to host USCH in San Juan. As a result, multiple hotel blocks will be available for attendees. While not ideal, it was the only way to bring the meeting to Puerto Rico. You must register for the conference in order to gain access to the block. Rooms will be set aside for scholarship recipients.


Most attendees will stay in one of two hotels. The Sheraton Puerto Rico is the host hotel and is located next to the convention center. Rooms at the Sheraton are $179 per night (plus taxes). We also have a block at the Caribe Hilton. This hotel just reopened; it was destroyed by Hurricane Maria in 2017. Rooms at the Hilton are $199 per night (plus taxes). The Hilton is located on the water a little further from the convention center. Buses will be provided to get people from the Hilton to the convention center. Hotel rooms are limited, so please register early.
For people needing less expensive accommodations, NMAC recommends Airbnb. On that site we found many reasonable places to stay near the convention center. Rooms and whole apartments can be found for $65 per night (plus taxes and fees). Unfortunately, San Juan is hurting for business. Air travel and accommodations are very reasonable. There is a direct flight out of DCA that is less than $300 (r/t). Our goal to bring economic development is real. In the near future, we will provide a list of local vendors for exhibitor and sponsors. Our hope is that everyone uses local companies, The people and businesses in San Juan need our help.
2020 Plenaries
- HIV in the Latinx Communities. This will be a Spanish language plenary with simultaneous English translation on the screens.
- Gilead Plenary
- Federal Update
- Proof of Concept that Biomedical HIV Prevention Works
The Opening honors Puerto Rico in food, decor, speakers, and language. It will represent the diversity of Puerto Ricans and Latinx who are working to end the HIV epidemic. This will be a Spanish language plenary with English translation on the large screens as a crawl at the bottom of the screen. It will feature Puerto Rican Salsa and Bomba y Plena music
2020 Workshops
 There will be a Spanish language track of workshops. In fact, the Call for Abstracts is in both English and Spanish. One of the new tracks is on Geriatric HIV Services. As PLWH age, it is time to relook at the mix of services our movement provides. During the early days, no one could have imagined the need for these services.
There will be a Spanish language track of workshops. In fact, the Call for Abstracts is in both English and Spanish. One of the new tracks is on Geriatric HIV Services. As PLWH age, it is time to relook at the mix of services our movement provides. During the early days, no one could have imagined the need for these services.
Child Care
NMAC will again provide child care. Like geriatric HIV services, child care was not on our radar in the early days. Now so many HIV positive people have children. It is a joy and honor to provide child care for them.
Opening Reception
The folks in PR are having real financial challenges, so it is not reasonable for NMAC to ask them to cover the same expenses as a typical host city. The host committee will be asked to put together the reception’s program that highlights the many cultures of Puerto Rico. NMAC is still trying to figure out how to cover the cost of food.
Guayaberas Shirts
 NMAC staff will wear Guayaberas on the first full day of USCH. A guayabera is a traditional Cuban shirt. The origin story tells of a poor countryside seamstress sewing large patch-pockets onto her husband’s shirts for carrying guava from the field. NMAC staff will wear guayaberas to honor the history and legacy of this shirt. We will put the 2020 theme, Luchando Por Nuestras Vida, on the back of the shirt.
NMAC staff will wear Guayaberas on the first full day of USCH. A guayabera is a traditional Cuban shirt. The origin story tells of a poor countryside seamstress sewing large patch-pockets onto her husband’s shirts for carrying guava from the field. NMAC staff will wear guayaberas to honor the history and legacy of this shirt. We will put the 2020 theme, Luchando Por Nuestras Vida, on the back of the shirt.
Scholarships
The scholarship section will go live on March 3. Last year we had challenges and many constituents were not happy with the results. This year NMAC has committed to double the number of A&B scholarships. However, given the number of applications we receive (more than 1,200), most people will be turned down. Do not depend on a USCH scholarship, Try to find other ways to get to the meeting. The website will share alternative ways to support your travel.
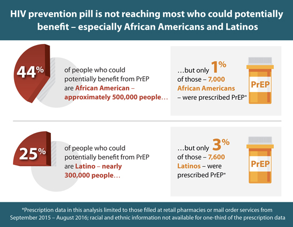
In our efforts to end HIV we must value and honor the cultures of the communities we are trying to reach. HIV impacts very specific communities. These are not general campaigns trying to reach everyone; these are targeted efforts. While the geographic targets are most obvious, within the 57 jurisdictions there are additional targets needed to end the epidemic. Understanding the values and cultures of the communities hardest hit by HIV is key to our success.
See you in October.
Paul Kawata