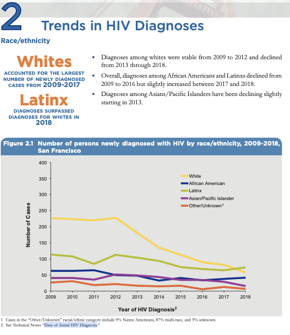
| While the Latinx community makes up 15% of the total population of SF, they are now the majority of new HIV cases. While this is only one year of data, what are the lessons? Can the shift in demographics for SF’s new HIV cases be attributed to the differences in PrEP uptake? About 18% of the people on PrEP in San Francisco are Latinx versus 16% for Asians, 9% for African Americans, 43% for White, and 19% for other.
Or maybe the surge in Latinx cases has more to do with the economics of the city. San Francisco has the highest density of billionaires of any city in the world. Economics are pushing African Americans and Latinx out. In a city that is set-up for the rich, what happens to poor people, particularly poor people living with HIV? NMAC’s concern is that this economic divide will end the HIV epidemic in rich communities while the poor are left to fend for themselves.
This will be the challenge for ending the HIV epidemic (EHE) plans. While we need to significantly increase the number of people on PrEP in all communities, plans need to target the communities that have eluded previous efforts. With Latinx PLWH making up the majority of new HIV cases in SF, are the majority of HIV services for the newly diagnosed provided by Latinx providers? Are there Latinx leaders in key administration positions in community-based organizations, health centers and the health department? Is San Francisco ready to manage this demographic shift in its HIV epidemic?
 All jurisdictions building EHE plans must look at how they are working with and including the Latinx community. Plans are required to have comprehensive community consultations with all the communities highly impacted by HIV. Disruptive innovation asks that we don’t bring the same faces to the table. Our efforts must reach beyond the status quo because we have to enroll communities that have eluded previous efforts. All jurisdictions building EHE plans must look at how they are working with and including the Latinx community. Plans are required to have comprehensive community consultations with all the communities highly impacted by HIV. Disruptive innovation asks that we don’t bring the same faces to the table. Our efforts must reach beyond the status quo because we have to enroll communities that have eluded previous efforts.
Reaching the Latinx community means having leaders from the Latinx communities planning and facilitating the meetings that target their community. The same holds true for all community consultations: leaders from the designated community should be in the driver’s seat. This is where the solution gets tough, as certain people and communities must let go of power.
Often I am not the right person to speak up. Understanding your privilege means understanding that you don’t have to speak first. In fact, sometimes you don’t have to speak at all. Just because you can doesn’t mean you should. There are too many in our movement, me included, who think we have the answers. This is why ending the epidemic will be a true test of our leadership. Will men let women speak? Can the cisgender community share leadership with transgender and gender non-conforming individuals? Can African Americans, Latinx, American Indians, Alaska Natives, Asians, and Pacific Islanders work together and not be pitted against each other? And what about White people?
 While these issues are so much bigger than HIV, they are central to our EHE plans. Can our movement expand to incorporate gay men of color, Black women, the transgender/gender non-conforming community, and people who use drugs into leadership positions? That’s what it’s going to take to end HIV: sharing power and letting other people lead. While these issues are so much bigger than HIV, they are central to our EHE plans. Can our movement expand to incorporate gay men of color, Black women, the transgender/gender non-conforming community, and people who use drugs into leadership positions? That’s what it’s going to take to end HIV: sharing power and letting other people lead.
Yours in the struggle,
Paul Kawata
30 Years of Service

|