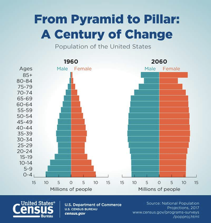
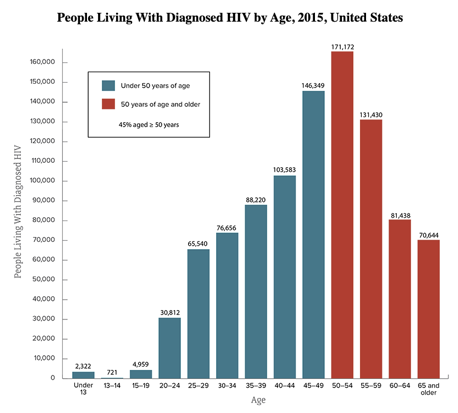
As of 2020, the CDC estimates that there are 770,000 adults over 50 living with HIV/AIDS in the US. That’s 70% of all people living with the virus with estimates that 24% of PLWHA have lived with the virus since before 1996. While some of the aging issues overlap there are differences that matter. As of 2020, the CDC estimates that there are 770,000 adults over 50 living with HIV/AIDS in the US. That’s 70% of all people living with the virus with estimates that 24% of PLWHA have lived with the virus since before 1996. While some of the aging issues overlap there are differences that matter.
 At NMAC, we are particularly concerned about the intersection of race and aging. Older black and Latinx people are more than twice as likely to not have supplemental Medicare insurance as their white counterparts. Black Medicare beneficiaries have higher levels of morbidity than their white counterparts. They also report lower levels of office visits and more inpatient, emergency room, and nursing home visits. Given the racial demographics of HIV, not only do we have to address issues of aging, but also the impact that race plays on aging with HIV. At NMAC, we are particularly concerned about the intersection of race and aging. Older black and Latinx people are more than twice as likely to not have supplemental Medicare insurance as their white counterparts. Black Medicare beneficiaries have higher levels of morbidity than their white counterparts. They also report lower levels of office visits and more inpatient, emergency room, and nursing home visits. Given the racial demographics of HIV, not only do we have to address issues of aging, but also the impact that race plays on aging with HIV.
 As I mentioned multiple times, Dr. Redfield has recommended using disruptive innovation to solve the challenges within EHE plans. Since we need to keep PLHIV/AIDS in care and on meds for the rest of their lives and the majority of this community are over 50, EHE plans must comprehensively address this challenge. NMAC recommends the following: As I mentioned multiple times, Dr. Redfield has recommended using disruptive innovation to solve the challenges within EHE plans. Since we need to keep PLHIV/AIDS in care and on meds for the rest of their lives and the majority of this community are over 50, EHE plans must comprehensively address this challenge. NMAC recommends the following:
- EHE Plans must explicitly address the HIV service mix for older PLHIV/AIDS
- When CDC/HRSA/HHS do joint final reviews of the G-57 plans, they must ensure comprehensive geriatrics HIV services are included in every plan.
- HRSA/HAB need to develop a list of services that all Ryan White providers should make available to serve the aging HIV community.
- CDC should ensure that a portion of the PrEP programming specifically outreaches to sexually active older Americans, especially people who have sex with folks from communities that are highly impacted by HIV.
- SAMHSA should put together a strategic plan to address the mental health issues facing long term HIV survivors.
- HUD should create a list of geriatric HIV components to be built into all HOPWA housing and the entire HUD portfolio.
- All plans to EHE must look at the intersection of aging and race.
The biomedical solution to ending the HIV epidemic is complex because it needs to speak to very specific communities with very specific needs. There is not a generic one size fits all solution. HIV Long-Term Survivors—women and men living with HIV for over 30 to 40 years face unique challenges not shared by people who acquired HIV after 1996 or so. What I appreciate most about the administration’s EHE plan is that it leaves the power with the jurisdictions. They get to determine the priorities and solutions. NMAC hopes they will use the new funding to build a comprehensive mix of HIV services that both reaches communities that were missed in previous efforts and speaks to the communities that are living longer with HIV/AIDS.
 To achieve the latter, the HIV service mix must prioritize older PLHIV/AIDS and sexually active older Americans who could benefit from PrEP. Older people in the United States are more likely than younger people to have late-stage HIV infection at the time of diagnosis, which means they start treatment late and possibly suffer more immune-system damage. Late diagnoses can occur because health care providers may not always test older people for HIV infection. To achieve the latter, the HIV service mix must prioritize older PLHIV/AIDS and sexually active older Americans who could benefit from PrEP. Older people in the United States are more likely than younger people to have late-stage HIV infection at the time of diagnosis, which means they start treatment late and possibly suffer more immune-system damage. Late diagnoses can occur because health care providers may not always test older people for HIV infection.
I know we don’t want to think about grandma having sex, but all you have to do is look at the rising STD rates for people over 55 (according to the CDC, gonorrhea rose 164% among American over 55 from 2014-2018, while cases of syphilis rose 120% and chlamydia rose 86% for this community) to see that she is having a good time.
Yours in the struggle,
Paul Kawata
Learning and Struggling To Be Proud Senior Citizen

|