|
|||
| ESCALATE is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) and the Minority HIV/AIDS Fund as part of a financial assistance award totaling $1,600,906.100 percentage funded by HRSA/HHS. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HRSA/HHS, or the U.S. Government. |

Dear Harold
|
|||
|
HIV Long Term Survivors Front and Center
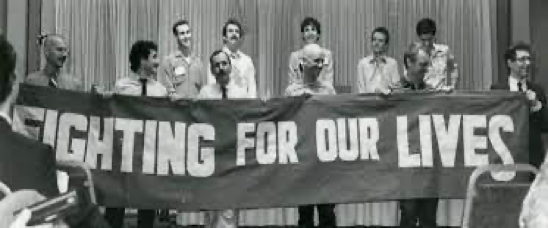
By Moisés Agosto-Rosario, NMAC Director of Treatment
 NMAC celebrates and honors HIV Long-Term HIV Long Term Survivors (HLTS) by raising awareness of their needs, issues, and journeys. For those who lived through the early days of the HIV epidemic, AIDS at 40 years is the future we never imagined. Our lives were full of uncertainties and fear. We were afraid of the possibility of being the next one to get sick and die. We took care of our friends and served our community fearlessly. We created HIV services by responding to our HIV+ brothers and sisters’ needs; we organized and mobilized by forming coalitions like the People with AIDS Coalition (PWAC), Body Positive (BP), and the AIDS Coalition to Unleash the Power (ACT UP). We created national organizations in Washington DC to advocate with us. Organizations like the National Association of People with AIDS (NAPWA), the National Minority AIDS Council (NMAC), the American Foundation For AIDS Research (AmfAR), and the AIDS Action Council and Foundation (today known as AIDS United) developed an HIV policy plan. They lobbied Congress and the federal government for funding and better provision of services.
NMAC celebrates and honors HIV Long-Term HIV Long Term Survivors (HLTS) by raising awareness of their needs, issues, and journeys. For those who lived through the early days of the HIV epidemic, AIDS at 40 years is the future we never imagined. Our lives were full of uncertainties and fear. We were afraid of the possibility of being the next one to get sick and die. We took care of our friends and served our community fearlessly. We created HIV services by responding to our HIV+ brothers and sisters’ needs; we organized and mobilized by forming coalitions like the People with AIDS Coalition (PWAC), Body Positive (BP), and the AIDS Coalition to Unleash the Power (ACT UP). We created national organizations in Washington DC to advocate with us. Organizations like the National Association of People with AIDS (NAPWA), the National Minority AIDS Council (NMAC), the American Foundation For AIDS Research (AmfAR), and the AIDS Action Council and Foundation (today known as AIDS United) developed an HIV policy plan. They lobbied Congress and the federal government for funding and better provision of services.
We shook government institutions through direct action, demonstrating against the government silence and inaction, pushing them to do the right thing. We became scientists and, with knowledge, demanded drugs into bodies and had a tangible impact on the development of HIV medicines. We created principles to empower ourselves and assert our right to “be involved at every level of decision-making and specifically serve on the boards of directors of provider organizations” and “not to be labeled as “victims,” a term which implies defeat.” I can go on and list the challenges and successes of the HIV community through the past 40 years with long-term survivors front and center. We are the reason we have treatment that has impacted our lifespan, allowing us to live longer and healthy lives. Long-term survivors should always be the foundation and the guiding principle for anyone in the HIV movement advocating or providing services.
Those of us aging with HIV and over 50 (HIV50+) are now the community’s elders. The HIV professional field and political movement were created by us and for us. Sadly, today it seems that we have been forgotten, and many of the elder HIV long-term survivors that once were warriors today are alone and in isolation. Our first HIV warriors are the long-term survivors we honor today and the first group of HIV+ people aging and over the age of 50. HLTS need science and research to understand the biology and medical treatment of aging with HIV, and health care that addresses multi-morbidities and develops standards of care and provision of services appropriate for this aging community. Today is a day to honor and reflect on what has been and will continue to be the role and contribution of the HIV 50+/HLTS. It is a day to renew our commitment to people living with HIV/AIDS (PLWHA), learn and implement the Denver Principles; it is a day to recognize and facilitate and empower PLWHA to be at the decision-making tables, as it should be. Long-term survivors are the guiding principle and light to illuminate the path and the action we take to end the HIV epidemic.
40 Years of HIV
|
|||||
|

vCROI Community Recap Recent Data on HIV and Aging
NMAC Stands With Billy Porter
Following is a statement from NMAC Executive Director Paul Kawata on “Pose” star Billy Porter’s disclosure of his HIV status.

“NMAC applauds Billy Porter on his disclosure of his HIV status. At NMAC, we know how much stigma around HIV cripples our ability to end the epidemic. It’s what keeps people from talking with their partners about HIV. It’s what keeps people from protecting themselves because they don’t feel worthy. It’s what keeps people away from doctors, clinics, and testing sites. And it perpetuates feelings of shame and deepens depression and poor self-esteem. As an award-winning actor, the lead of a hit TV show, and a gay man of color, Billy Porter’s disclosure can have a big impact on HIV stigma, particularly in communities of color where it remains a major obstacle.
“We are so happy that this disclosure is bringing him a sense of relief and release of pain and trauma. Billy is an amazing actor, singer, dancer, and now role model for people of color living with or affected by HIV. We look forward to having him as a partner in the fight against HIV.”
NMAC leads with race to urgently fight for health equity and racial justice to end the HIV epidemic in America. Since 1987, NMAC has advanced our mission through a variety of programs and services, including: a public policy education program, national and regional training conferences, a treatment and research program, numerous electronic and print materials, and a website: www.nmac.org. NMAC also serves as an association of AIDS service organizations, providing valuable information to community-based organizations, hospitals, clinics, and other groups assisting individuals and families affected by the HIV epidemic.
I Made A Mistake
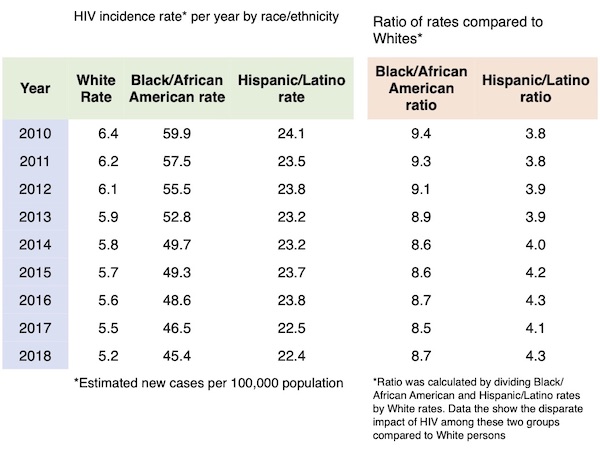
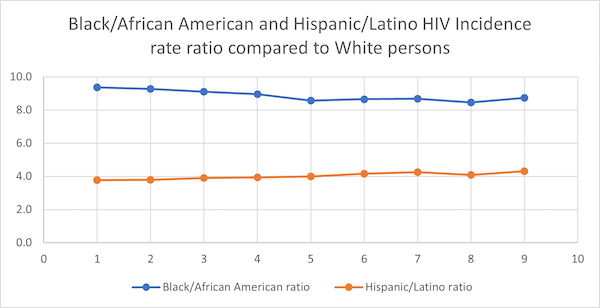
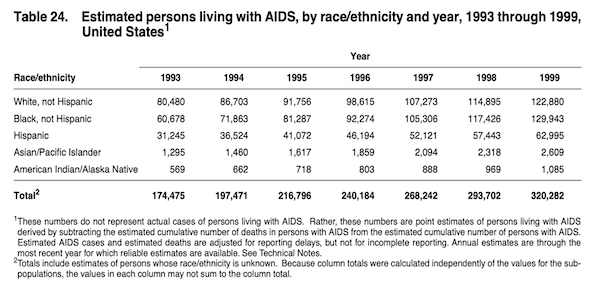
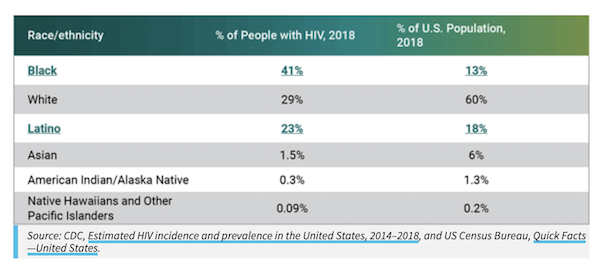
I made a mistake in last week’s piece on the Minority AIDS Initiative (MAI). I believe good leadership is owning your mistakes and working to fix it. As you probably know, I am not an epidemiologist. However, NMAC will always follow the data and the science and the data I shared last week did not capture the impact that MAI has by race/ethnicity. Here is the corrected data that I received:
|
|||
|
BLOC En Español Comes to Texas
NMAC proudly announces the Building Leaders of Color (BLOC) en español virtual training program for Texas this June 21- 25, 2021 (10am-3PM CST). The main goal of BLOC en español is to increase the meaningful participation of Persons of Color with HIV (PWH) who are prepared to engage in leadership roles and activities related to HIV service delivery in their communities. The training will be facilitated in Spanish.
BLOC en español is designed in Spanish language to provide language justice and cultural humility to the Latinx community. The program also utilizes NMAC’s new learning management system (the HIV-E virtual platform) and a tutorial prior will be provided. BLOC en español’s learning objectives include:
- Leadership development for community engagement including defining traits and characteristics of leaders
- Developing a community lens on the forms of stigmas including enacted and layered stigma
- What are and how to use health numeracy, measurement tools, and patient support tools for planning
- Developing skills to effectively be engaged in surveillance, evaluation, calculations, data analysis, and performance measurements as a community leader
- Increase knowledge of the Ryan White HIV/AIDS Program and other planning bodies for involvement
- Elaborate leadership opportunities considering self-care
- Develop individualized action goals and goal statements for seeking leadership opportunities
After completing the program participants are encouraged to engage in the planning process with a local community group serving persons living with HIV such as, Ryan White HIV/AIDS Program planning bodies. The program is available for all (PLH) who reside in Houston, Texas whose primary language is Spanish. The Ryan White HIV/AIDS Program recipients are highly encouraged to apply. The program will recruit up to 30 participants.
Apply by Sunday, June 20th, 2021, using the following link: https://www.surveymonkey.com/r/HTX2021
For more information contact: Cora Trelles Cartagena (She/Ella), HIV Systems Coordinator at ccartagena@nmac.org or 202-870-0481. Please visit us at nmac.org, Twitter/Facebook: @NMACCommunity and Instagram: @nmachiv.
This Building Leaders of Color (BLOC) en español is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of a financial assistance award totaling $550,000 with 100% percentage funded by HRSA/HHS. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HRSA/HHS, or the U.S. Government.
Who Benefits from Minority AIDS Initiative (MAI) Funding?
|
|||||||||||
|
ESCALATE and ELEVATE Coming This Summer
This summer, NMAC will officially launch our Ending Stigma through Collaboration and Lifting All to Empowerment (ESCALATE) and Engage Leadership through Employment, Validation, and Advancing Transformation and Equity (ELEVATE) training programs. For more information on these programs, please contact Charles Shazor at cshazor@nmac.org or Terrell Parker at tparker@nmac.org.
ESCALATE
Purpose
![]() The purpose of the ESCALATE training program is to facilitate transformative and relational change in Ryan White HIV/AIDS Programs and the communities they serve through deepening awareness of and practices for cultural humility amongst Persons with HIV (PWH) and RWHAP providers.
The purpose of the ESCALATE training program is to facilitate transformative and relational change in Ryan White HIV/AIDS Programs and the communities they serve through deepening awareness of and practices for cultural humility amongst Persons with HIV (PWH) and RWHAP providers.
The ESCALATE program will train participants in the 57 jurisdictions identified in Ending the HIV Epidemic: A Plan for America (EHE) to recognize and address HIV stigma with a particular focus on transgender/gender nonconforming individuals, men who have sex with men, and the Black/African American community. NMAC works in partnership with NORC at and the University of Chicago, Abt Associates, and TRX Development Solutions.
Central to the focus of ESCALATE are community involvement and cultural competency. HIV stigma is a multi-dimensional social issue with various complexities and nuances. Understanding the needs of community is critical. The ESCALATE program engages subject matter experts from impacted communities through the curriculum design. This ensures “buy in” and also guarantees the success of the program. MIPA or the Meaningful Involvement of People Living with HIV and AIDS challenges the idea of creating a service or program without the intentional inclusion and advice of PWH.
Goals
- Create an environment of psychological safety for persons with HIV and RWHAP providers to deepen their understanding and practices of cultural humility
- Effectively engage in difficult dialogues with communities and institutions about the influence of race, power, privilege, and identity
- Identify stereotypes, prejudice, and discrimination as forms of bias while learning to recognize and manage unconscious thoughts and feelings influencing behaviors
Objectives
- Create a shared mental model of cultural humility in theory and in practice
- Define the “American Dilemma” in the context of race and health care delivery
- Define intersectionality and demonstrate how it impacts outcomes for marginalized people and groups
- Introduce the multidimensional model of privilege as a tool to disrupt the single-target group approach
- Introduce and utilize de-biasing tools and strategies
- Use reflection and self-critique to explore participant attitudes and beliefs
- Review individual and organizational strategies to disrupt implicit bias in health care settings
ESCALATE Training Participants
- Persons with HIV (PWH) and RWHAP Recipient/Subrecipients Partners (Parts A, B, C, & D)
ELEVATE
Purpose
![]() The purpose of the ELEVATE program is to expand the participation of people living with HIV (PLHIV) in the HIV workforce, planning councils, and other community leadership roles. ELEVATE builds on the achievements of HRSA and Ryan White HIV/AIDS Program (RWHAP) training programs and incorporates their features into a single project. NMAC works in partnership with the JSI Research Training Institute, Inc., the Association of Nurses in AIDS Care (ANAC), and the Latino Commission on AIDS (LCOA). Program evaluation will be provided by NMAC’s long term evaluation partner, ICF an internationally recognized evaluation firm.
The purpose of the ELEVATE program is to expand the participation of people living with HIV (PLHIV) in the HIV workforce, planning councils, and other community leadership roles. ELEVATE builds on the achievements of HRSA and Ryan White HIV/AIDS Program (RWHAP) training programs and incorporates their features into a single project. NMAC works in partnership with the JSI Research Training Institute, Inc., the Association of Nurses in AIDS Care (ANAC), and the Latino Commission on AIDS (LCOA). Program evaluation will be provided by NMAC’s long term evaluation partner, ICF an internationally recognized evaluation firm.
The ELEVATE program is modeled on NMACs previous HRSA-supported training program, Building Leaders of Color (BLOC) and will integrate the BLOC curriculum with other training programs sponsored by HRSA including: JSI’s “Community HIV/AIDS TA Training” (CHATT) and “Access Care Engagement Technical Assistance Center” (ACE TA Center); the Center for Quality Improvement and Innovation’ s “Training Consumers on Quality Plus;” and Boston University School of Social Work’s “Improving Access to Care: Using Community Health Workers to Improve Linkage and Retention in Care (Among People of Color).” ELEVATE integrates the unique contributions of each of these past programs to provide a state-of-the-art, comprehensive training program for the leadership and inclusion of PLHIV in community decision making bodies and the agencies that serve PWH.
Goals
- Increase the number of PWH meaningfully involved in the planning, delivering, and improving of RWHAP services
- Build the capacity of PWH to be meaningfully involved in community planning for HIV prevention, care, and treatment services
- Build the capacity of PWH to be meaningfully involved in clinical quality management (CQM) activities
- Build the capacity of PWH to be meaningfully involved in the delivery of HIV prevention, care, and treatment services
- Develop individualized action plans to increase engagement and involvement in the planning, delivering, and improving of RWHAP services
Audience
Persons with HIV (PWH) aligned with a RWHAP Recipient or Subrecipient
- Employed by RWHAP
- Members of Planning Bodies or Planning Councils
- Members of Consumer, Community, & Patient Advisory Boards
- Directors from the Boards of RWHAP
- Members of Clinical Quality Management Teams or Committees
- Other PWH aligned with a RWHAP seeking greater involvement
ESCALATE is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) and the Minority AIDS Initiative as part of a financial assistance award totaling $1,600,906. ELEVATE is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of a financial assistance award totaling $796,749 respectively with 100 percentage funded by HRSA/HHS. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HRSA/HHS, or the U.S. Government.