
By the end of June, the Supreme Court will hand down decisions on two cases that could have profound impacts on our world. Happy Pride! After overturning Roe, we should not be surprised. While the cases are not HIV specific, these decisions could hurt communities highly impacted by HIV. The two cases include:
- 303 Creative LLC vs. Elenis
- Affirmative Action
303 Creative LLC vs. Elenis is about freedom of speech and public accommodation. Does the owner of 303 Creative LLC have the right to publish the following on her websites, “I will not be able to create websites for same-sex marriages or any other marriage that is not between one man and one woman. Doing that would compromise my Christian witness and tell a story about marriage that contradicts God’s true story of marriage.”
Since we already lost the case of the Christian baker who did not want to make wedding cakes for a same-sex couples, there is precedence to discriminate. What makes this different is her desire to put this statement on her corporate webpage. Does her right to free speech supersede local ordinances against discrimination in public accommodation?
Make no mistake, the wording is different, but the sentiment is the same. People of color have a long history fighting these actions, and they seldom end well. If she is allowed to post this statement, does that open the door for other businesses to follow? Does it stop with same sex marriages? What about others who compromise her Christian witness, for example, Muslims or atheists? While I am not concerned about a single website developer, I am very concerned that this seems to be part of a larger concerted effort to weaponize my community. When SCOTUS flipped, it seemed like an inflection point to ramp-up their campaign of hate. This year there are multiple court cases, hundreds of pieces of legislation, and too many elected officials leaning into the culture wars. It can’t be a coincidence. As they rewrite the role of the courts in our democracy, it becomes a pathway for the minority to control and “bring America back.”

 You may not remember, but there was a time when funeral homes regularly refused to cremate people who died from AIDS. Hospitals turned away or made people living with HIV so uncomfortable as to make them leave. Laws to stop discrimination in public accommodations were written for a reason. If she wins, then we, the LGBTQ community, will in fact be second class citizens. People and corporations will not only legally be allowed to discriminate against us, but they can also explicitly note that in their communications. Most large corporations will continue to support the LGBTQ community; however, this decision further divides our country and stokes the flames of discrimination and hate. It also could set the precedent that hate speech overrides local or state laws protecting access to public accommodations.
You may not remember, but there was a time when funeral homes regularly refused to cremate people who died from AIDS. Hospitals turned away or made people living with HIV so uncomfortable as to make them leave. Laws to stop discrimination in public accommodations were written for a reason. If she wins, then we, the LGBTQ community, will in fact be second class citizens. People and corporations will not only legally be allowed to discriminate against us, but they can also explicitly note that in their communications. Most large corporations will continue to support the LGBTQ community; however, this decision further divides our country and stokes the flames of discrimination and hate. It also could set the precedent that hate speech overrides local or state laws protecting access to public accommodations.
 Affirmative Action is also under review by this court. While most of the press is focused on higher education, it is important to understand the implications this decision could have on efforts to end the HIV epidemic in America. The Minority AIDS Initiative was created in the late ’90s to build organizations and infrastructure in communities of color to address the epidemic. At that time, people of color were disproportionately impacted by HIV.
Affirmative Action is also under review by this court. While most of the press is focused on higher education, it is important to understand the implications this decision could have on efforts to end the HIV epidemic in America. The Minority AIDS Initiative was created in the late ’90s to build organizations and infrastructure in communities of color to address the epidemic. At that time, people of color were disproportionately impacted by HIV.
The Bush Administration used a previous Supreme Court ruling on Affirmative Action to gut the MAI. Funding priorities went from minority led nonprofits to minority serving nonprofits. That simple change decimated many of the minority led HIV organizations. To this day it is still being used as the reason change is impossible. An unintended consequence is that 10 years after the MAI was gutted, people of color became the majority of new cases and the majority of people living with HIV.
 Black Lives Matter moved the dialogue about race in America. It was a reckoning that both opened important discussions and scared others to “take back America.” NMAC, along with the Latino Commission on AIDS, SF Community Health Center, and Southern AIDS Coalition are working with Congresswoman Maxine Waters and Congresswoman Barbara Lee to bring a portion of the MAI back to its original congressional intent. This year we got so close, and all of us remain committed to this effort. We will continue to work with the Congressional Black, Hispanic, Asian, LGBTQ+ Equality and HIV caucuses.
Black Lives Matter moved the dialogue about race in America. It was a reckoning that both opened important discussions and scared others to “take back America.” NMAC, along with the Latino Commission on AIDS, SF Community Health Center, and Southern AIDS Coalition are working with Congresswoman Maxine Waters and Congresswoman Barbara Lee to bring a portion of the MAI back to its original congressional intent. This year we got so close, and all of us remain committed to this effort. We will continue to work with the Congressional Black, Hispanic, Asian, LGBTQ+ Equality and HIV caucuses.
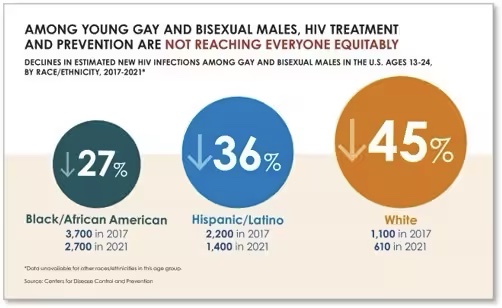
The HIV movement knows race matters. You see it in our programs, services, and staff. In many ways we are the model for diversity. So why does our work fail to reach so many in need? What are the systemic changes needed to bend the curve of new HIV infections. Recently CDC data showed a significant decrease in the cases of HIV, unfortunately those decreases were not across the board.
 HIV sits at the intersection of so many critical and divisive challenges in America. Community based nonprofits and health departments are to be applauded for their ability to hire people with lived experience. This means many of your employees come from the communities hardest hit by HIV. They/we expect you to stand up and fight for community and to fight for our shared values and humanity, especially as we are weaponized for political gain. The pain is not just out there, it is also in our house. America feels like it is overrun with homophobia, racism, sexism, and transphobia. Not only are the consumers we need to reach in trauma, but our staffs are in trauma. I am in trauma.
HIV sits at the intersection of so many critical and divisive challenges in America. Community based nonprofits and health departments are to be applauded for their ability to hire people with lived experience. This means many of your employees come from the communities hardest hit by HIV. They/we expect you to stand up and fight for community and to fight for our shared values and humanity, especially as we are weaponized for political gain. The pain is not just out there, it is also in our house. America feels like it is overrun with homophobia, racism, sexism, and transphobia. Not only are the consumers we need to reach in trauma, but our staffs are in trauma. I am in trauma.
 Allowing her to write on our webpage, “I will not be able to create websites for same-sex marriages or any other marriage that is not between one man and one woman. Doing that would compromise my Christian witness and tell a story about marriage that contradicts God’s true story of marriage.” is the equivalent of No F@gs Allowed. Not only does it legalize trauma and discrimination, but it also supersedes any state or city public accommodation laws.
Allowing her to write on our webpage, “I will not be able to create websites for same-sex marriages or any other marriage that is not between one man and one woman. Doing that would compromise my Christian witness and tell a story about marriage that contradicts God’s true story of marriage.” is the equivalent of No F@gs Allowed. Not only does it legalize trauma and discrimination, but it also supersedes any state or city public accommodation laws.
Yours in the Struggle,

 I was that little boy who could not hide his gayness. My mouth opens, and a purse falls out. I was born this way. From an early age, I loved Barbra Streisand, the Supremes, and musicals much to the bafflement of my parents. You could say it was in my DNA. That’s why I know being gay is not a choice. Who would choose a life fill with stigma, discrimination, and threats of violence? At the same time, you can’t taste freedom and not want to be free. As Americans, we innately understand this proposition. Being gay is who I was meant to be and praying to God would not change that reality.
I was that little boy who could not hide his gayness. My mouth opens, and a purse falls out. I was born this way. From an early age, I loved Barbra Streisand, the Supremes, and musicals much to the bafflement of my parents. You could say it was in my DNA. That’s why I know being gay is not a choice. Who would choose a life fill with stigma, discrimination, and threats of violence? At the same time, you can’t taste freedom and not want to be free. As Americans, we innately understand this proposition. Being gay is who I was meant to be and praying to God would not change that reality.
 There is a whole generation coming of age in the 2023 era of trauma and vilification of the LGBTQ community. It is real shit right now and will only get worse with the Presidential election next year. I worry for the future. Then I remember that we stand on the shoulders of heroes. To the 16-year-old boy, I say look at me now. This picture was taken when I was a marshal at DC Pride. Our history documents our strength. Overcoming adversity is in our DNA. It took a long time and many tears for that scared boy to become this outrageous Queen. While I am still a work in progress, coming out and speaking my truth changed the trajectory of my life. Happy Pride everyone!
There is a whole generation coming of age in the 2023 era of trauma and vilification of the LGBTQ community. It is real shit right now and will only get worse with the Presidential election next year. I worry for the future. Then I remember that we stand on the shoulders of heroes. To the 16-year-old boy, I say look at me now. This picture was taken when I was a marshal at DC Pride. Our history documents our strength. Overcoming adversity is in our DNA. It took a long time and many tears for that scared boy to become this outrageous Queen. While I am still a work in progress, coming out and speaking my truth changed the trajectory of my life. Happy Pride everyone!

















