 NMAC urgently fights for racial justice and health equity. Health equity means everyone has access to quality healthcare and the medications needed to live long healthy and happy lives. Healthcare is a right and not a privilege. Justice is about prioritizing those communities with the greatest need. The opening plenary for the 2019 Biomedical HIV Prevention Summit will ask the question, “Can We End the HIV Epidemic in Women, Particularly Black Women?” There was some push back to that announcement: “What about Latinas? What about all women? Why only hold out Black Women?” The fact is that Black women account for 60% of all the women living with HIV in the United States. This question highlights the racial justice struggle to end the HIV epidemic. NMAC fights for equal access to HIV services and meds for all women, and we want justice for Black women. The burden of the HIV epidemic on Black women calls out for justice.
NMAC urgently fights for racial justice and health equity. Health equity means everyone has access to quality healthcare and the medications needed to live long healthy and happy lives. Healthcare is a right and not a privilege. Justice is about prioritizing those communities with the greatest need. The opening plenary for the 2019 Biomedical HIV Prevention Summit will ask the question, “Can We End the HIV Epidemic in Women, Particularly Black Women?” There was some push back to that announcement: “What about Latinas? What about all women? Why only hold out Black Women?” The fact is that Black women account for 60% of all the women living with HIV in the United States. This question highlights the racial justice struggle to end the HIV epidemic. NMAC fights for equal access to HIV services and meds for all women, and we want justice for Black women. The burden of the HIV epidemic on Black women calls out for justice.
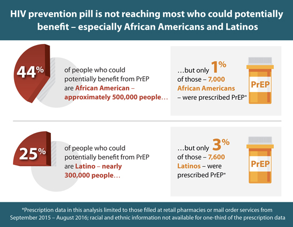 NMAC wants everyone to have access to PrEP. When 75% of the people on PrEP are white, it becomes an issue of racial justice. PrEP programs that reach highly-impacted communities of color must come from and be culturally responsive to those communities. Unfortunately, it is not just a matter of switching white faces for people of color. PrEP programs that reach highly-impacted communities of color must come from and be culturally responsive to those communities.
NMAC wants everyone to have access to PrEP. When 75% of the people on PrEP are white, it becomes an issue of racial justice. PrEP programs that reach highly-impacted communities of color must come from and be culturally responsive to those communities. Unfortunately, it is not just a matter of switching white faces for people of color. PrEP programs that reach highly-impacted communities of color must come from and be culturally responsive to those communities.
We also need to talk about justice for the transgender community. As long as the CDC continues to classify transgender men and women with gay men, we will never end the HIV epidemic in the ![]() transgender community. How can you end what you do not know? If we don’t know the number of transgender men and women living with HIV, how will this initiative know it is successful? NMAC questions the scientific accuracy of CDC’s HIV epidemiological profiles because of this long-held practice. At its core, this is not good public health practice and something that the CDC can and should change.
transgender community. How can you end what you do not know? If we don’t know the number of transgender men and women living with HIV, how will this initiative know it is successful? NMAC questions the scientific accuracy of CDC’s HIV epidemiological profiles because of this long-held practice. At its core, this is not good public health practice and something that the CDC can and should change.
 HIV funding must address equity and justice. NMAC believes that all communities should have the resources needed to end the HIV epidemic; however, as a matter of justice, we believe the resources need to prioritize the communities that are hardest hit by HIV. In the United States, gay men share the largest burden of HIV. As the federal government looks to target resources geographically, HIV prevention and care efforts need to target the communities with the greatest burden of HIV: Black/Latinx/American Indian gay men, Black cisgender heterosexual women, people of transgender experience, and drug users. Funding priorities need to follow the epidemiological profile of that jurisdiction.
HIV funding must address equity and justice. NMAC believes that all communities should have the resources needed to end the HIV epidemic; however, as a matter of justice, we believe the resources need to prioritize the communities that are hardest hit by HIV. In the United States, gay men share the largest burden of HIV. As the federal government looks to target resources geographically, HIV prevention and care efforts need to target the communities with the greatest burden of HIV: Black/Latinx/American Indian gay men, Black cisgender heterosexual women, people of transgender experience, and drug users. Funding priorities need to follow the epidemiological profile of that jurisdiction.
This is where the fight starts.
We are all hopeful and thankful for new resources, but will the money get to the organizations that can reach the communities hardest hit by HIV? NMAC hopes the G-57 jurisdictions will put out requests for funding that speaks to community and their strengths. Too often awards are won by organizations who can afford expensive grant writers, but could never reach the most affected subpopulations. NMAC will work with the G-57 to identify best practices that support community responses.
Agencies and health departments that implement new programs should be required to hire people from the communities that effort hopes to reach. If you want to reach the transgender community, then you need to hire transgender people. If you want to reach black women, then you need to hire black women. If you want to reach drug users, then you need to hire people with experience using drugs. If you want to reach people over 50 living with HIV, then you need to hire people over 50 living with HIV.
While this might seem self-evident, you would be surprised how often it does not happen. Now is the time to take a census of who works at the health department, community health center or community-based organization. Does staff reflect, represent, and have senior staff from the communities the work needs to reach? NMAC does not mean to imply that you need to get rid of anyone but, when there are new hires, who gets the job? Now is the time to correct any past challenges and build a work force that can speak the communities this effort needs to reach.
 Our work to end the epidemic must be viewed through a racial justice and health equity lens. It is more than retention in care and adherence to meds. It’s retention in care and adherence to meds in the communities that are hardest hit by HIV. NMAC will fight to ensure that all communities have access to the health care and the medications needed to live long healthy and happy lives. We will also fight for justice to make sure that the communities hardest hit by HIV are prioritized. The color of your skin should never be a determining factor for who acqires HIV or any other disease. In the words of the late Congressmen Elijah Cummings, “we are better than this!”
Our work to end the epidemic must be viewed through a racial justice and health equity lens. It is more than retention in care and adherence to meds. It’s retention in care and adherence to meds in the communities that are hardest hit by HIV. NMAC will fight to ensure that all communities have access to the health care and the medications needed to live long healthy and happy lives. We will also fight for justice to make sure that the communities hardest hit by HIV are prioritized. The color of your skin should never be a determining factor for who acqires HIV or any other disease. In the words of the late Congressmen Elijah Cummings, “we are better than this!”
Yours in the struggle,
Paul Kawata
30 Years of Service
