Today the administration released their recommendations for the 2021 federal budget that included $716 million for the Ending the HIV Epidemic (EHE) efforts. The Budget includes: $371 million for CDC to reduce new HIV infections; $302 million for Health Resources and Services Administration (HRSA) to deliver HIV care through the Ryan White HIV/AIDS Program and to supply testing, evaluation, prescription of PrEP, and associated medical costs through the Health Centers program; $27 million to the Indian Health Service (IHS) to tackle the epidemic in American Indian and Alaska Native communities; and $16 million for the National Institutes of Health (NIH) for evaluation activities to identify effective interventions to treat and prevent HIV.
Congress does not typically pass a budget in an election year and more than likely we have a Continuing Resolution (CR). NMAC and the many partners with a Washington presence will fight like hell for the new funding, but there are forces beyond HIV that will shape the end result. All is not lost, because often a budget gets passed after the election.
NMAC is a small agency working to have a huge impact. While we are thankful to the administration for the much-needed funding, it is difficult, if not impossible to reconcile our concerns about other parts of the budget and the policies of the administration. Our movement looks to NMAC to lead with race as we fight for health equity and racial justice for the communities hardest hit by HIV. We try to walk this very thin tightrope, but it’s not easy and there are many landmines.
 Over the next few months, the federal government’s EHE efforts will grant hundreds of millions of dollars to the 57 target jurisdictions and beyond. This initiative is the direct result of NMAC and many other partners working together to move our work beyond the maintenance phase that had become the new normal. Now our job is to make sure the new funding gets to community because that is where we will end the epidemic.
Over the next few months, the federal government’s EHE efforts will grant hundreds of millions of dollars to the 57 target jurisdictions and beyond. This initiative is the direct result of NMAC and many other partners working together to move our work beyond the maintenance phase that had become the new normal. Now our job is to make sure the new funding gets to community because that is where we will end the epidemic.
Our EHE work must be based on our values. NMAC leads with race to end the HIV epidemic. Our values shape the way we fight. They are the foundation for the principles that guide our work and the best practices to end the epidemic. Here are some values that we hope jurisdictions will incorporate into their plans,
- Race matters.
- People Living with HIV/AIDS must be prioritized, especially PLWH/A who have fallen out of care and off their meds.
- Jurisdictional plans must reach communities highly impacted by HIV who were missed in previous efforts.
- Reaching hard to reach communities requires the buy-in and leadership from the people we are trying to reach.
- New hires to implement EHE plans should come from these communities.
- Funding should always follow the data; however, we need better data on the transgender community.
- CDC needs to stop classifying the transgender community with men who have sex with men.
- Community led planning and community evaluation needs to be built into the process.
- Scientifically proven interventions are key to this effort. These interventions must work at a scale to reach the large numbers targeted in the plan.
- Fighting stigma and ending HIV criminalization is core to supporting people living with HIV/AIDS.
- STDs and Hepatitis are key pathways to ending the HIV epidemic.
 NMAC is concerned that some jurisdictions will repeat the same programs and miss key communities. While we need to expand programs that are successful, we must also acknowledge that large segments of the communities highly impacted by HIV are not being reached. This is particularly true for gay men of color, black women, the transgender community, and people who use drugs. NMAC respects Dr. Redfield’s call for Disruptive Innovation to end the epidemic. Like him, we believe there needs to be disruptive innovation in order to reach communities that don’t trust the status quo.
NMAC is concerned that some jurisdictions will repeat the same programs and miss key communities. While we need to expand programs that are successful, we must also acknowledge that large segments of the communities highly impacted by HIV are not being reached. This is particularly true for gay men of color, black women, the transgender community, and people who use drugs. NMAC respects Dr. Redfield’s call for Disruptive Innovation to end the epidemic. Like him, we believe there needs to be disruptive innovation in order to reach communities that don’t trust the status quo.
Talking To CDC
 Two weeks ago, I wrote about the number of staff that are in CDC’s Division of HIV/AIDS Prevention. After talking with CDC, it is important for me to correct the record. The Division of HIV/AIDS Prevention (DHAP) at CDC does not have 800 full time employees:
Two weeks ago, I wrote about the number of staff that are in CDC’s Division of HIV/AIDS Prevention. After talking with CDC, it is important for me to correct the record. The Division of HIV/AIDS Prevention (DHAP) at CDC does not have 800 full time employees:
- DHAP has the authority to hire 554 full time permanent employees at headquarters and 20 in the field for direct assistance.
- However, currently, the Division has approximately 425 full time permanent employees at headquarters and 13 in the field.
CDC let me know that they need a fully resourced headquarters operations to reach the goals of EHE and to perform the following types of work:
- Running a state-of-the-art laboratory.
- Developing, planning, implementing, managing, and evaluating strategies for HIV prevention with state and local public health departments, community-based organizations, and other nongovernmental organizations.
- Monitoring HIV trends and providing the epidemiological investigation and analysis required to support informed prevention efforts and public health action at federal, state, and community levels.
- Conducting HIV outbreak detection and response.
- Conducting research to ensure that proven and innovative tools and interventions are available to prevent HIV.
- Developing, evaluating, producing, and disseminating science-based communications on HIV for the public, providers, and persons at risk of HIV infection to ensure they have the tools needed to protect themselves or their patients from HIV infection.
- Investing in the next generation of public health professionals.
- Improving HIV prevention workforce by increasing the knowledge, skills, technology, and infrastructure needed to implement and sustain science-based, culturally appropriate HIV prevention interventions and strategies.
CDC also said that 9% of the funding will stay at the agency for operations, or around $12.6 million. I appreciate their transparency about funding and hope it will continue. NMAC’s concern was not about the specific number of employees, but rather the building of a government bureaucracy vs. getting the money to the field. NMAC’s goal is to make sure money and programming gets to community because we believe that is where it can make the biggest difference. NMAC and CDC agreed to monthly calls to build better collaboration.
NMAC and CDC agreed to monthly calls to build better collaboration. The first call will be coordinated by NMAC’s Center to End the HIV Epidemic in conjunctions with the 57 jurisdictions prioritized in the EHE plan. This will be an opportunity for them to interact with colleagues from other regions and to ask questions to the CDC.
 With the HRSA and CDC funding announcements on the street, NOW is the time to make sure the money gets to where it can make the most difference. If we don’t speak up, decisions will be made that may or may not include community.
With the HRSA and CDC funding announcements on the street, NOW is the time to make sure the money gets to where it can make the most difference. If we don’t speak up, decisions will be made that may or may not include community.
NMAC is a small agency working to change the world. We focus on race and its impact on HIV. It’s easy to feel like Don Quixote. Are we chasing after windmills or changing the world? Sometimes they look the same. This may be an impossible dream, but we are still praying for a cure and a vaccine. NMAC believes there is a world without HIV/AIDS, and we are fighting to make that dream real.
Yours in the struggle,
Paul Kawata



 The first round of funding did not go as planned for too many. Will this next round be any better? The Partnership’s lobbyist David H. Reid and his colleague Matthew McKissick will be online to talk about the new round of support and how nonprofits can apply.
The first round of funding did not go as planned for too many. Will this next round be any better? The Partnership’s lobbyist David H. Reid and his colleague Matthew McKissick will be online to talk about the new round of support and how nonprofits can apply.














 We invite all people living with HIV/AIDS to join the call and share their experience of living with HIV during COVID-19. I know this is something that HHS and HRSA are tracking. Please join the call to share your concerns with Harold. It’s too soon to have real scientific studies, so we are looking for anecdotes for how PLHIV are coping.
We invite all people living with HIV/AIDS to join the call and share their experience of living with HIV during COVID-19. I know this is something that HHS and HRSA are tracking. Please join the call to share your concerns with Harold. It’s too soon to have real scientific studies, so we are looking for anecdotes for how PLHIV are coping. NMAC uses
NMAC uses 
 The purpose of the webinars is to discuss relief for nonprofits via the
The purpose of the webinars is to discuss relief for nonprofits via the 

 shows that lessons learned fighting HIV help to inform the response to COVID-19.
shows that lessons learned fighting HIV help to inform the response to COVID-19.

 Since many people will now be working from home, it is also important to learn from Long Term Survivors about the reality that isolation caused by the virus (either one) can lead to depression. As we think about how to work from home, please do not forget the behavioral health challenges. We are asking everyone to isolate themselves for an undetermined amount of time. This presents a multitude of issues. If interacting with people was the best solution to ending the social isolation,how do you do that in the age of COVID-19? There are real mental health issues that must be managed when putting people in isolation for extended periods of time.
Since many people will now be working from home, it is also important to learn from Long Term Survivors about the reality that isolation caused by the virus (either one) can lead to depression. As we think about how to work from home, please do not forget the behavioral health challenges. We are asking everyone to isolate themselves for an undetermined amount of time. This presents a multitude of issues. If interacting with people was the best solution to ending the social isolation,how do you do that in the age of COVID-19? There are real mental health issues that must be managed when putting people in isolation for extended periods of time.
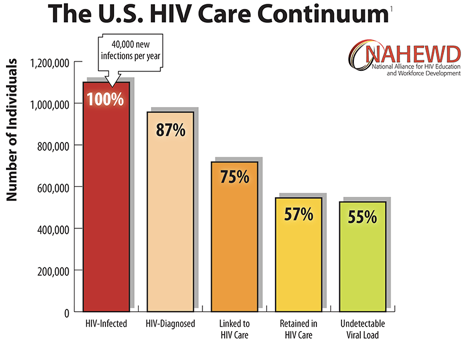
 Not only do we need to hire people living with HIV/AIDS, we also need to make sure the new hires reflect the diversity of the local epidemic in terms of race, gender, sexual orientation and people with trans experience. Peer to peer outreach has always been shown to be the most effective way to touch hard to reach communities. From NMAC’s perspective, who gets hired will make the difference between ending the epidemic versus staying the course with 40,000 new cases every year.
Not only do we need to hire people living with HIV/AIDS, we also need to make sure the new hires reflect the diversity of the local epidemic in terms of race, gender, sexual orientation and people with trans experience. Peer to peer outreach has always been shown to be the most effective way to touch hard to reach communities. From NMAC’s perspective, who gets hired will make the difference between ending the epidemic versus staying the course with 40,000 new cases every year. Over the next weeks, NMAC is going to put together a sign-on letter to HHS, CDC, and HRSA asking them to review, evaluate, and update the HIV service mix to meet the needs of an aging population of PLHIV/AIDS. NMAC will bring 15 people over 50 living with HIV to AIDS Watch to both train and to make sure this important voice is at the table. While in Washington, NMAC will seek a meeting with Harold Phillips, Dr. Laura Cheever, and Dr. Jono Mermin to talk about all the issues, challenges, and opportunities that ending the epidemic provides for people living with HIV/AIDS. The administration may not fully understand the central role at PLHIV/AIDS play in ending the epidemic, so it is our movement’s responsibility to both educate and nudge them.
Over the next weeks, NMAC is going to put together a sign-on letter to HHS, CDC, and HRSA asking them to review, evaluate, and update the HIV service mix to meet the needs of an aging population of PLHIV/AIDS. NMAC will bring 15 people over 50 living with HIV to AIDS Watch to both train and to make sure this important voice is at the table. While in Washington, NMAC will seek a meeting with Harold Phillips, Dr. Laura Cheever, and Dr. Jono Mermin to talk about all the issues, challenges, and opportunities that ending the epidemic provides for people living with HIV/AIDS. The administration may not fully understand the central role at PLHIV/AIDS play in ending the epidemic, so it is our movement’s responsibility to both educate and nudge them.